LYME TRANSMISSION & MAINTENANCE: Various Transmission Methods
|
Including examination of I. uriae (seabird)
& I. auritulus (bird) ticks |
Including examination of H. longicornis
(scrub/bush) & H. bispinosa ticks |

|
Various Transmission Methods:
In This Section: *Blood Sucking insects (other than ticks) *Contact Transmission *Human to Human Transmission (Sexual and Mother to Baby) *Organ and Blood Donation |
Lyme Borreliosis is described as a vector-borne disease as it is spread via the bite of arachnids (ticks). It should also be noted that there are various other methods of transmission. Some of these methods are confirmed, with others subject to speculation and requiring further research.
1. Evidence that blood sucking insects (other than ticks) are able to transmit Lyme disease;
2. Contact (urine passed) transmission has been noted in mice, and;
3. Human to human transmission : sexual and mother to baby (vertical).
These three areas areas are outlined briefly below. How Lyme is transmitted and maintained within the environment and the well known ability of the tick to spread Lyme disease / Borreliosis in discussed in more detail on the 'Lyme Transmission & Maintenance' page of this site.
A fourth method of transmission, Organ and Blood Donation, is to be added to this segment. It will be updated with information and references in the near future. For immediate further reading on Borrelia (and other) infections acquired due to organ donation see: Donor-Derived Infections in Solid Organ Transplantation
1. Evidence that blood sucking insects (other than ticks) are able to transmit Lyme disease;
2. Contact (urine passed) transmission has been noted in mice, and;
3. Human to human transmission : sexual and mother to baby (vertical).
These three areas areas are outlined briefly below. How Lyme is transmitted and maintained within the environment and the well known ability of the tick to spread Lyme disease / Borreliosis in discussed in more detail on the 'Lyme Transmission & Maintenance' page of this site.
A fourth method of transmission, Organ and Blood Donation, is to be added to this segment. It will be updated with information and references in the near future. For immediate further reading on Borrelia (and other) infections acquired due to organ donation see: Donor-Derived Infections in Solid Organ Transplantation
Blood sucking insects (other than ticks)
In clinical cases of Lyme disease, biting flies (1-3), mosquito’s (3, 4) and mites (5) are suggested to have been responsible for the infection. The Borrelia bacteria has been found in: numerous species of mites (6); fleas (6-8) ; biting flies, ie: bot flies, deer flies, horse flies (6,7, 9-11) ; and mosquito’s (8, 9, 11-14), indicating that these insects are capable of maintaining the bacteria and are potential vectors.
In clinical cases of Lyme disease, biting flies (1-3), mosquito’s (3, 4) and mites (5) are suggested to have been responsible for the infection. The Borrelia bacteria has been found in: numerous species of mites (6); fleas (6-8) ; biting flies, ie: bot flies, deer flies, horse flies (6,7, 9-11) ; and mosquito’s (8, 9, 11-14), indicating that these insects are capable of maintaining the bacteria and are potential vectors.
Contact transmission
Borrelia spirochetes have been found in the urine of infected dogs (15,16), horses (17,18), cattle (18) and mice (19,20). Studies on mice have found that the spirochetes in urine remained viable for 18-24 hours and concluded that “Urine may provide a method for contact non-tick transmission of B. burgdorferi in natural rodent populations particularly during periods of nesting and/or breeding” (19: pg 40). Evidence for direct contact transmission has been demonstrated in mice (20). These findings suggest that further research is needed to ascertain whether, like the spirochete that causes Leptospirosis, the Borrelia spirochete is able to spread by the urine of infected animals to humans.
Borrelia spirochetes have been found in the urine of infected dogs (15,16), horses (17,18), cattle (18) and mice (19,20). Studies on mice have found that the spirochetes in urine remained viable for 18-24 hours and concluded that “Urine may provide a method for contact non-tick transmission of B. burgdorferi in natural rodent populations particularly during periods of nesting and/or breeding” (19: pg 40). Evidence for direct contact transmission has been demonstrated in mice (20). These findings suggest that further research is needed to ascertain whether, like the spirochete that causes Leptospirosis, the Borrelia spirochete is able to spread by the urine of infected animals to humans.
Human to human transmission : Sexual Transmission
There is no direct evidence for sexual transmission, although spirochetes have been found in semen (21), suggesting that it is a possibility. Lyme disease has also been likened to another spirochetal disease, syphilis, which is a sexually transmittable infection (22).
There is no direct evidence for sexual transmission, although spirochetes have been found in semen (21), suggesting that it is a possibility. Lyme disease has also been likened to another spirochetal disease, syphilis, which is a sexually transmittable infection (22).
Human to human transmission : Mother to Baby
The possibility of placental transmission is acknowledged, although there are mixed reports regarding exactly what health risk congenital Lyme disease poses to the foetus/newborn. A brief dialogue of various positions is presented below:
Allan MacDonald (1989) notes that adverse reactions, such as foetal death and cortical blindness, have been associated with gestational Lyme disease and suggests the need for further research in order to ascertain whether the associations are co-incidental or related to the infection (23).
MacDonald AB (1989) Gestational Lyme borreliosis. Implications for the fetus:
Abstract: “Great diversity of clinical expression of signs and symptoms of gestational Lyme borreliosis parallels the diversity of prenatal syphilis. It is documented that transplacental transmission of the spirochete from mother to fetus is possible... Autopsy and clinical studies have associated gestational Lyme borreliosis with various medical problems including fetal death, hydrocephalus, cardiovascular anomalies, neonatal respiratory distress, hyperbilirubinemia, intrauterine growth retardation, cortical blindness, sudden infant death syndrome, and maternal toxemia of pregnancy. Whether any or all of these associations are coincidentally or causally related remains to be clarified by further investigation”.
The possibility of placental transmission is acknowledged, although there are mixed reports regarding exactly what health risk congenital Lyme disease poses to the foetus/newborn. A brief dialogue of various positions is presented below:
Allan MacDonald (1989) notes that adverse reactions, such as foetal death and cortical blindness, have been associated with gestational Lyme disease and suggests the need for further research in order to ascertain whether the associations are co-incidental or related to the infection (23).
MacDonald AB (1989) Gestational Lyme borreliosis. Implications for the fetus:
Abstract: “Great diversity of clinical expression of signs and symptoms of gestational Lyme borreliosis parallels the diversity of prenatal syphilis. It is documented that transplacental transmission of the spirochete from mother to fetus is possible... Autopsy and clinical studies have associated gestational Lyme borreliosis with various medical problems including fetal death, hydrocephalus, cardiovascular anomalies, neonatal respiratory distress, hyperbilirubinemia, intrauterine growth retardation, cortical blindness, sudden infant death syndrome, and maternal toxemia of pregnancy. Whether any or all of these associations are coincidentally or causally related remains to be clarified by further investigation”.
The International Disease Society of America (IDSA) guidelines downplay any risk, associated with Lyme, and conclude that “there is little evidence that a congenital Lyme disease syndrome occurs” (24).
The International Disease Society of America (IDSA): “Some practitioners prescribe a 10–14-day course of prophylactic amoxicillin for pregnant women after I.Scapularis tick bites, because case reports have suggested that Lyme disease during pregnancy may be associated with adverse outcomes for the fetus. However, a large body of data from clinical and epidemiologic studies suggest that favorable outcomes can be expected when pregnant women with Lyme disease are treated with standard antibiotic regimens. Indeed, there is little evidence that a congenital Lyme disease syndrome occurs” (Pg 10).
The International Disease Society of America (IDSA): “Some practitioners prescribe a 10–14-day course of prophylactic amoxicillin for pregnant women after I.Scapularis tick bites, because case reports have suggested that Lyme disease during pregnancy may be associated with adverse outcomes for the fetus. However, a large body of data from clinical and epidemiologic studies suggest that favorable outcomes can be expected when pregnant women with Lyme disease are treated with standard antibiotic regimens. Indeed, there is little evidence that a congenital Lyme disease syndrome occurs” (Pg 10).
The Centre for Disease Control (CDC) notes that while “Lyme disease can be dangerous for your unborn child”, and “may lead to infection of the placenta and may possibly lead to stillbirth” (25,26), it follows the IDSA guidelines that “favorable outcomes can be expected when pregnant women with Lyme disease are treated with standard antibiotic regimen” ; Contrary to this statement, there are reports of adverse outcomes, including the death of newborns, with (27) or without (28) antibiotic treatment of the mother.
CDC Publications include :
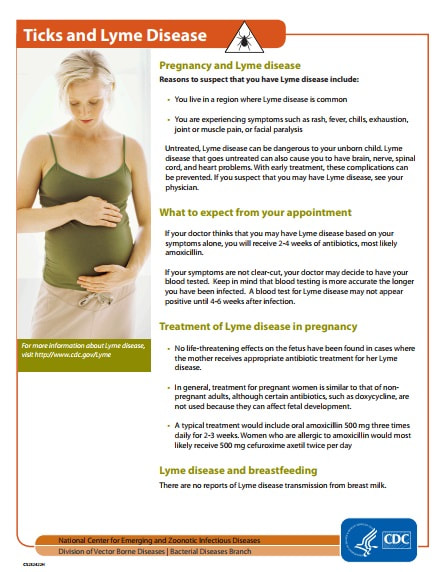
Pregnancy Fact Sheet: “Untreated, Lyme disease can be dangerous to your unborn child. Lyme disease that goes untreated can also cause you to have brain, nerve, spinal cord, and heart problems”. See publication reproduced in the pictures below, or on the CDC Website
Lyme Disease Resource Brochure: “Prevention and early diagnosis of Lyme disease are important during pregnancy. Rarely, Lyme disease acquired during pregnancy may lead to infection of the placenta and may possibly lead to stillbirth. Studies of women infected during pregnancy have found that there are no negative effects on the fetus when the mother receives appropriate antibiotic treatment for her Lyme disease ".
See the relevant section of the publication reproduced in the pictures below. The full publication can be viewed on the CDC Website
CDC Publications include :
Pregnancy Fact Sheet: “Untreated, Lyme disease can be dangerous to your unborn child. Lyme disease that goes untreated can also cause you to have brain, nerve, spinal cord, and heart problems”. See publication reproduced in the pictures below, or on the CDC Website
Lyme Disease Resource Brochure: “Prevention and early diagnosis of Lyme disease are important during pregnancy. Rarely, Lyme disease acquired during pregnancy may lead to infection of the placenta and may possibly lead to stillbirth. Studies of women infected during pregnancy have found that there are no negative effects on the fetus when the mother receives appropriate antibiotic treatment for her Lyme disease ".
See the relevant section of the publication reproduced in the pictures below. The full publication can be viewed on the CDC Website
Pictures Below: Left: CDC Pregnancy Fact Sheet ; Right: CDC Lyme Disease Resource Brochure, section on Pregnancy and Lyme
|
|
|

National Institutes of Health puts it short and sweet: “If you are pregnant, be especially careful to avoid ticks in Lyme disease areas because you can pass on the infection to your unborn child”. (NIH Publication, Page 15). The NIH publication does not appear to be available online in any location.
I have reproduced the page with this quote on it below.
I have reproduced the page with this quote on it below.
Picture Gallery Below : 4 pages from the NIH Publication: National Institutes of Health, U.S. Department of Health and Human Services (2008). Lyme Disease: The Facts, the Challenge.
1st page: NIH Publication Page 15 which notes in the second paragraph: "If you are pregnant, be especially careful to avoid ticks in Lyme disease areas because you can pass on the infection to your unborn child”.
Pages 2-4: The first three pages of the NIH publication : The cover page, the publication details and the index.
1st page: NIH Publication Page 15 which notes in the second paragraph: "If you are pregnant, be especially careful to avoid ticks in Lyme disease areas because you can pass on the infection to your unborn child”.
Pages 2-4: The first three pages of the NIH publication : The cover page, the publication details and the index.
Further information on Congenital Lyme disease can also be seen at: John Drulle MD Lyme Website
References: LYME TRANSMISSION: The Debates
(1) Luger SW (1990) Lyme Disease Transmitted by a Biting Fly. N Engl J Med; 322(24):175 http://www.ncbi.nlm.nih.gov/pubmed/2342543
(2) Herzer P, Wilske B, Preac-Mursic V, Schierz G, Schattenkirchner M and Zollner N (1986) Lyme arthritis: clinical features, serological, and radiographic findings of cases in Germany. Klin Wochenschr ; 64(5):206-15 http://www.ncbi.nlm.nih.gov/pubmed/3702279
(3) Doby JM, Chastel C, Couatarmanac'h A, Cousanca C, Chevrant-Breton J, Martin A, Legay B and Guiguen C (1985) Etiologic and epidemiologic questions posed by erythema chronicum migrans and Lyme disease. Apropos of 4 cases at the Regional HospitalCenter, Rennes. Bull Soc Pathol Exot Filiales; 78(4):512-25 http://www.ncbi.nlm.nih.gov/pubmed/4075471
(4) Hard S (1966) Erythema chronicum migrans (Afzelii) associated with mosquito bite. Acta Dermato-Venereol;46:473-476 www.ncbi.nlm.nih.gov/pubmed/4163724
(5) Badalian LO, Kravchuk LN, Sergovskaia VD, Belousova VS and Minina AP (1994) The neurological syndromes in Lyme disease in children. Zh Nevrol Psikhiatr Im S S Korsakova; 94(3):3-6 http://www.ncbi.nlm.nih.gov/pubmed/7975984
(6) Pokorny P (1989) Incidence of the spirochete Borrelia burgdorferi in arthropods (Arthropoda) and antibodies in vertebrates (Vertebrata). Cesk Epidemiol Mikrobiol Imunol; 38 (1): 52-60 http://www.ncbi.nlm.nih.gov/pubmed/2646031
(7) Anderson JF and Magnarelli LA (1984) Avian and mammalian hosts for spirochete-infected ticks and insects in a Lyme disease focus in Connecticut. Yale J Biol Med ;57(4):627-41. http://www.ncbi.nlm.nih.gov/pubmed/6516460
(8) Hubalek Z, Halouzka J and Juricova Z (1998) Investigation of haematophagous arthropods for borreliae--summarized data, 1988-1996. Folia Parasitol (Praha);45(1):67-72.http://www.ncbi.nlm.nih.gov/pubmed/9516997
(9) Magnarelli LA, Anderson JF and Barbour AG (1986) The etiologic agent of Lyme disease in deer flies, horse flies, and mosquitoes. J Infect Dis 1986;154 (2) :355-8 http://www.ncbi.nlm.nih.gov/pubmed/2873190
(10) Stanek G, Flamm H, Groh V, Hirschl A, Kristoferitsch W, Neumann R, Schmutzhard E and Wewalka G (1987) Zentralbl Bakteriol Mikrobiol Hyg (A) ;263(3):442-9 http://www.ncbi.nlm.nih.gov/pubmed/3591096
(11) Magnarelli LA and Anderson JF (1988)Ticks and Biting Insects Infected with the Etiologic Agent of Lyme Disease, Borrelia burgdorferi. J Clin Microbiol: 26 (8): 1482-6 http://www.ncbi.nlm.nih.gov/pubmed/3170711
(12) Halouzka J, Wilske B, Stunzner D, Sanogo YO Hubalek (1999) Isolation of Borrelia afzelli from Overwintering Culex pipiens Biotype molestus Mosquitoes. 1999 Infection;27(4-5):275-7 http://www.ncbi.nlm.nih.gov/pubmed/10885843
(13) Zakovska A, Capkova L, Sery O, Halouzka J and Dendis M (2006) Isolation of Borrelia afzelli from overwintering Culex pipiens biotype molestus mosquitoes. Ann Agric Environ Med; 13 (2): 345-348 http://www.ncbi.nlm.nih.gov/pubmed/17199258
(14) Kosik-Bogacka DI, Juzna-Grygiel W and Jaborowska M (2007) Ticks and mosquitoes as vectors of Borrelia burgdorferi sl in the forested areas of Szczecin. Folia Biol (Krakow): 55(3-4): 143-6 http://www.ncbi.nlm.nih.gov/pubmed/18274258
(15) Grauer GF, Burgess FC, Cooley AJ and Hagee JH (1998) Renal lesions associated with Borrelia burgdorferi infection in a dog. J Am Vet Med Assoc; 193 (2) 237-239 http://www.ncbi.nlm.nih.gov/pubmed/3403355
(16) Cerri D, Farina R, Andreani E, Nuvoloni R, Pedrini A and Cardini G (1994) Experimental infection of dogs with Borrelia burgdorferi. Res Vet Sci; 57(2):256-8 http://www.ncbi.nlm.nih.gov/pubmed/7817018
(17) Burgess EC (1988) Borrelia burgdorferi infection in Wisconsin horses and cows. Ann N Y Acad Sci; ;539:235-43 http://www.ncbi.nlm.nih.gov/pubmed/3190095
(18) Manion TB, Khan, MI, Dinger J and Bushmich SL (1998) Viable Borrelia burgdorferi in the urine of two clinically normal horses. J Vet Diagn Invest 10 (2):196–199 http://www.ncbi.nlm.nih.gov/pubmed/9576355
(19) Bosler EM and Schultze TL (1986) The prevalence and significance of Borrelia burgdorferi in the urine of feral reservoir hosts. Zentralbl Bakteriol Mikrobiol Hyg A; 263(1-2):40–44 http://www.ncbi.nlm.nih.gov/pubmed/3577491
(20) Burgess EC, Amundson TE, Davis JP, Kaslow RA and Edelman R (1986) Experimental inoculation of Peromyscus spp. with Borrelia burgdorferi: evidence of contact transmission. Am J Trop Med Hyg; 35(2):355-359 http://www.ncbi.nlm.nih.gov/pubmed/3513648
(21) Recovery of Lyme Spirochetes by PCR in Semen Samples of Previously Diagnosed Lyme Disease Patients. Presented by Dr. Gregory Bach, at the International Scientific Conference on Lyme Disease, April, 2001 http://www.samento.com.ec/sciencelib/4lyme/recoveryoflyme.html
(22) Virginia Lyme site: https://sites.google.com/site/virginialyme/sexual
(23) MacDonald AB (1989) Gestational Lyme borreliosis. Implications for the fetus. Rheum Dis Clin North Am; 15(4):657-77
http://www.ncbi.nlm.nih.gov/pubmed/2685924
(24) The International Disease Society of America (IDSA) guidelines: The Clinical Assessment, Treatment, and Prevention of Lyme Disease, Human Granulocytic Anaplasmosis, and Babesiosis: Clinical Practice Guidelines by the Infectious Diseases Society of America. (Clinical Infectious Diseases 2006; 43:1089–134) http://cid.oxfordjournals.org/content/43/9/1089.full
(25) Centre for Disease Control: Lyme Disease; Pregnant Woman Fact Sheet : Accessed: February 2012 http://www.cdc.gov/lyme/resources/toolkit/factsheets/10_508_Lyme%20disease_PregnantWoman_FACTSheet.pdf
(26) Centre for Disease Control: Lyme Disease; Resource Brochure : Accessed: February 2012. Link updated 2017:
https://www.cdc.gov/lyme/resources/brochure/lymediseasebrochure.pdf
(27) Weber K, Bratzke HJ, Neubert U, Wilske B and Duray PH (1988) Borrelia burgdorferi in a newborn despite oral penicillin for Lyme borreliosis during pregnancy. Pediatr Infect Dis J; 7(4):286-9 http://www.ncbi.nlm.nih.gov/pubmed/3130607
Only the details of the journal article available at pubmed website (unless you have access): though J. Drulle writes about Weber et al’s findings
(1986) that were published (1988) in this article.
John Drulle MD Lyme Website: http://johndrullelymefund.org/wp-content/uploads/2012/02/Pregnancy-and-Lyme-Disease.pdf
(28) Schlesinger PA, Duray PH, Burke BA, Steere AC and Stillman MT (1985) Maternal-fetal transmission of the Lyme disease spirochete, Borrelia burgdorferi. Ann Intern Med; 103(1):67-8. http://www.ncbi.nlm.nih.gov/pubmed/4003991
Only the details of the journal article available at pubmed website: this article can be read in full via the
Canadian Lyme disease website : http://www.canlyme.com/Schlesinger_1985.pdf
(29) National Institutes of Health, U.S. Department of Health and Human Services (2008). Lyme Disease: The Facts, the Challenge (NIH Publication No. 08-7041). This Publication appears to have been removed from the National Institute of Health Website: http://www.niaid.nih.gov/topics/lymeDisease/Documents/lymedisease.pdf
The full publication can still be viewed (correct as at June 2012) at the Town of Boxborough, Massachusetts website: Update : NIH Publication has since been removed from this website also. Previously available : [ http://www.town.boxborough.ma.us/NIHLymeDisease.pdf ]
